
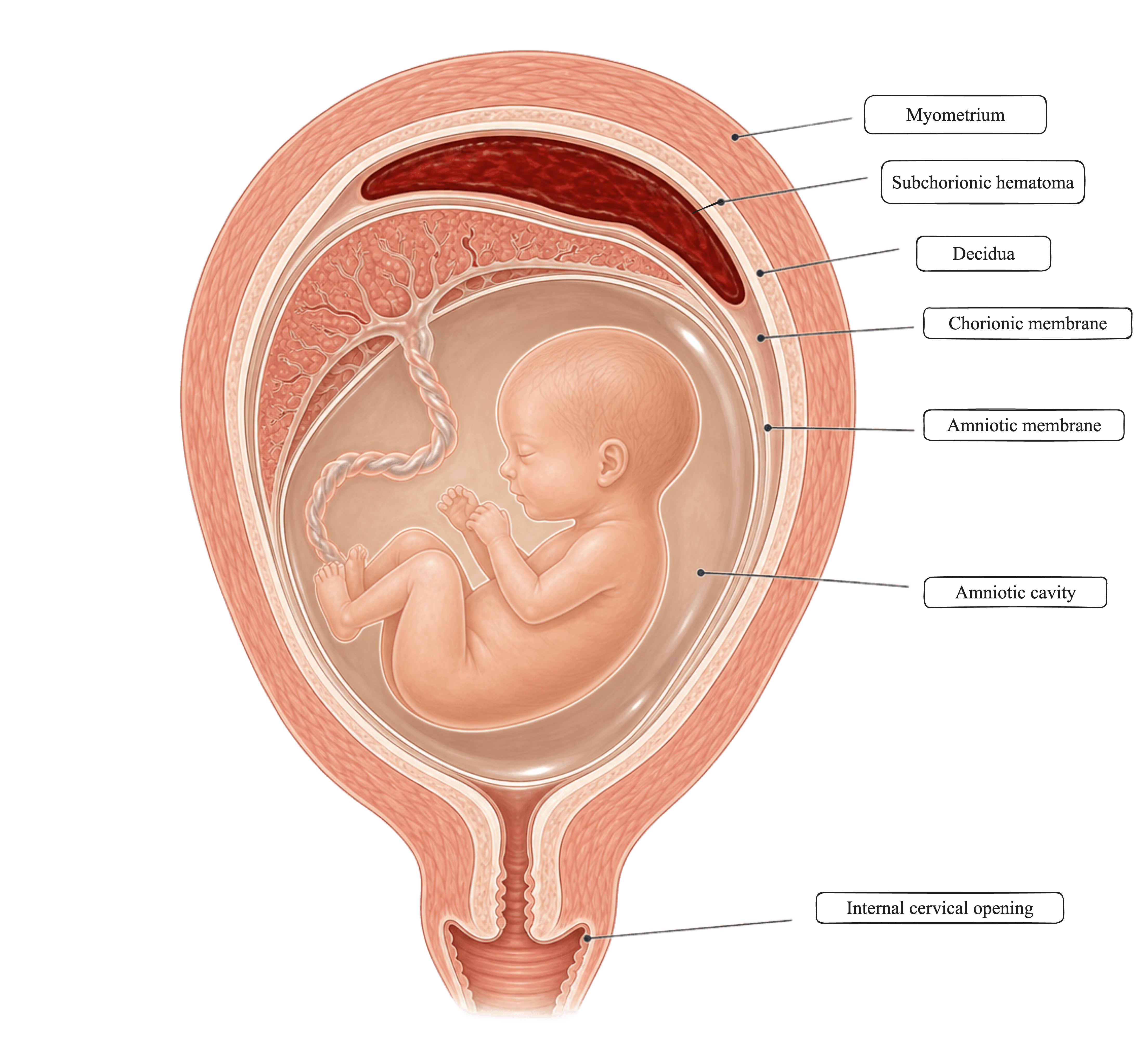
She is sixteen weeks pregnant. Spotting again this week, the second time. The ultrasound shows a subchorionic hematoma — eight by two-point-eight by three centimeters — stable from her hospitalization a few days ago. She is hemodynamically fine. Her labs are clean. I cannot fix this. I can only watch with her.
This is the part of obstetrics that does not make the headlines. We have the most advanced imaging in human history, and at sixteen weeks with a subchorionic bleed, my management plan is essentially the same as it would have been in 1965 — rest, follow-up, hope, and a conversation about how far she can fly. We can treat hemorrhage. We can treat preeclampsia. We can treat retained placenta. The bleed inside the uterine wall that may or may not absorb? We sit with it. And the patient sits with it longer than we do.
This is also a story about the evidence we never built. The Pregnancy Risk Assessment Monitoring System — the federal surveillance system that has, since 1987, asked roughly three thousand new mothers in each participating state what actually happened to them — is the kind of platform that could have, over thirty-eight years, told us whether closer follow-up changes the outcome for a patient like this. Whether her experience of the watching shapes her recovery. Whether the management I am offering her in 2026 is meaningfully different from the management offered in 1965. PRAMS does not regulate care. It does not tell me what to do. It is the long-running infrastructure that would, if asked the right questions, let me offer her something more than the same plan from sixty years ago.
That platform is being dismantled. The 2023 PRAMS dataset was cleaned and ready for release in March 2025. It has never been released. The team that would have released it was placed on administrative leave on April 1, 2025, and has not been rehired. The paperwork keeps moving through the system — Federal Register notices, OMB extension requests, the agency’s procedural shell — but the work the paperwork authorizes has not happened in over a year. The watching is the management plan today, in part, because we did not build the evidence to do better. And the system that could have built it is, by administrative action and without a vote, no longer building it.
The watching is the management plan because we did not build the evidence to do better — and the system that could have built it is, by administrative action without a vote, no longer building it.
I scheduled her follow-up close together. Not because the ultrasound will change anything — it almost certainly will not. I did it because the psychosocial weight of wait and see is its own clinical problem, even when the physiology is stable. Her not being alone in the watching is something I can do. The fear has a name. The plan has a rhythm. We will see each other every two weeks until this resolves or it does not.
What I can do, in addition to scheduling close follow-up, is chart this encounter with the kind of detail that PRAMS, when it existed, would have captured at the population level. I write the size of the hematoma. I write what she told me about the spotting — when it started, how heavy, what she was doing. I write her response to the conversation about flying. I write the psychosocial context — the fear, the pacing of the questions, the fact that she came alone. I do this not because the next ultrasound will change my plan, but because, in a federal environment that has stopped producing population-level surveillance, the only remaining record of what a sixteen-week pregnancy with a stable subchorionic bleed looks like in real time, in a real woman, is what individual clinicians write in their charts.
That is not a substitute for PRAMS. It cannot be. The platform PRAMS provided — sampling, weighting, comparability across states, decades of longitudinal trend — is the kind of infrastructure no number of well-documented charts can replace. But the chart is what is left. And when the surveillance system that documented maternal experience for thirty-eight years is dismantled by administrative action, the bedside record becomes the last remaining record. The watching becomes the data.
Tell her that the federal data system that could have produced better evidence is being dismantled. Patients can carry that. They are not protected by being told the evidence simply does not exist, when the more honest answer is that the evidence is being prevented. Naming the limit gives her something to do with the watching. And if she asks what she can do — the answer is that Congress already appropriated PRAMS in P.L. 119-75, signed into law on February 3, 2026.
The administration is refusing to staff the program Congress paid for. That is not an appropriations fight; it is an executive-branch enforcement fight. The Impoundment Control Act and the Administrative Procedure Act are the legal architecture. If she has a representative whose office takes constituent calls, the ask is not “fund PRAMS.” The ask is “enforce the appropriation.” That is a different conversation, with a different answer.
The watching is the care.